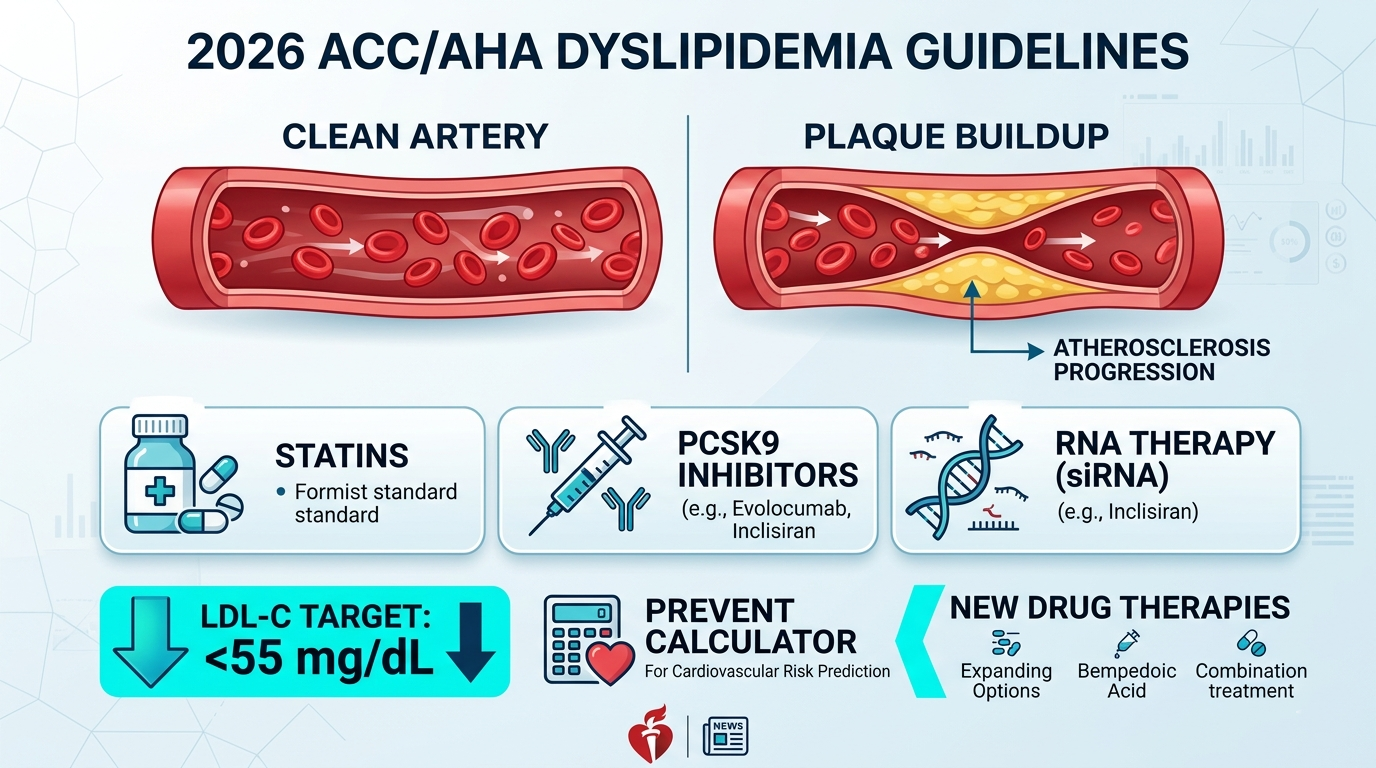
2026 ACC/AHA Dyslipidemia Guidelines: Everything Has Changed About How We Treat Cholesterol
A pharmacist-reviewed guide to the most significant update to cardiovascular prevention guidelines in a decade — new LDL targets, new risk calculator, new drugs, and what every patient should know.
Reviewed by a Registered Pharmacist | Source: JACC, Circulation, ACC, AHA | Published March 13, 2026
Introduction
On March 13, 2026, the American College of Cardiology (ACC) and the American Heart Association (AHA), alongside nine other leading medical societies, released the 2026 ACC/AHA Guideline on the Management of Dyslipidemia — the most comprehensive update to cardiovascular prevention guidelines in nearly a decade. This document replaces the 2018 AHA/ACC Guideline on Blood Cholesterol and overhauls how clinicians and patients should think about cholesterol, lipid risk, and the prevention of atherosclerotic cardiovascular disease (ASCVD).
The name change alone signals a paradigm shift — from ‘blood cholesterol’ to ‘dyslipidemias’ — acknowledging that elevated LDL is no longer the only lipid threat worth treating. Triglycerides, lipoprotein(a) [Lp(a)], and apolipoprotein B (ApoB) now share centre stage.
“We know 80% or more of cardiovascular disease is preventable and elevated LDL cholesterol is a major part of that risk. Lower LDL cholesterol for longer, just like lower blood pressure for longer, results in much greater protection against future heart attack and stroke risk.” — Roger Blumenthal, MD, FACC, FAHA, Chair of the 2026 Guideline Writing Committee, Johns Hopkins University
In this blog, we explore the 2026 ACC/AHA Dyslipidemia Guidelines — what changed, what it means for patients, the new drug options now recommended, and what every pharmacist needs to know before these guidelines reshape clinical practice.
What Is Dyslipidemia — and Why the New Guidelines Matter?
Dyslipidemia refers to abnormal levels of lipids in the blood — including elevated LDL cholesterol, elevated triglycerides, low HDL cholesterol, and high levels of atherogenic particles such as lipoprotein(a) and apolipoprotein B. These lipid abnormalities are a primary driver of atherosclerosis — the build-up of fatty plaques in artery walls — which ultimately causes heart attacks, strokes, and peripheral artery disease.
Cardiovascular disease (CVD) remains the world’s leading cause of death. The 2026 guidelines reflect a scientific consensus that the earlier, broader, and more precisely lipid abnormalities are treated, the greater the reduction in lifetime cardiovascular events.
| CVD deaths globally per year | Adults with dyslipidemia (US) | Heart attacks preventable with optimal LDL | Adults with elevated Lp(a) |
|---|---|---|---|
| 18 million+ | ~95 million | >80% | 1 in 5 |
Sources: WHO 2024; ACC/AHA 2026 Guideline; JACC March 2026
Prior guidelines (2018) focused almost exclusively on LDL-C and percentage reductions from statin therapy. The 2026 guidelines introduce specific numerical LDL targets, a brand-new risk calculator, universal Lp(a) testing, and a clearly mapped pharmacotherapy escalation pathway — representing the most practical guidance clinicians and pharmacists have received in over a decade.
Key Drug & Treatment Changes — What Are the 2026 Guidelines?
The 2026 ACC/AHA Guideline on the Management of Dyslipidemia is a comprehensive clinical document jointly published in JACC and Circulation. It is classified as a GLP (Guideline-Level Publication) with Class I, IIa, IIb, and III recommendations graded by level of evidence.
| Topic | 2018 Guideline | 2026 Guideline (NEW) |
|---|---|---|
| Risk Calculator | Pooled Cohort Equations (PCE) — 40–75 yrs, race-adjusted | PREVENT equations — 30–79 yrs, race-free, 10-yr + 30-yr estimates |
| LDL-C Targets | No specific targets; statin intensity-based | Specific targets restored: <55, <70, <100 mg/dL by risk tier |
| Scope | Blood Cholesterol (LDL focus) | Full Dyslipidemias: LDL + triglycerides + Lp(a) + ApoB |
| Lp(a) Testing | Selected high-risk patients only | Universal: every adult, once in a lifetime |
| ApoB Testing | Limited mention | Clear pathway: guide treatment in high-risk patients |
| Earliest Treatment | Age 40+ primary prevention focus | Children 9–11 screened; statins considered ≤ 30 yrs |
| Bempedoic Acid | Not included (post-2018 approval) | Formally incorporated in escalation pathway |
| Inclisiran | Not included (post-2018 approval) | Positioned after PCSK9 monoclonal antibodies |
| Triglycerides | Limited guidance | ≥150 mg/dL recognized as ASCVD risk; full treatment pathway |
| CAC Role | Tie-breaker, optional | Strengthened; opportunistic CT reporting encouraged |
Both statins and emerging non-statin therapies are incorporated under the new cardiovascular-kidney-metabolic (CKM) syndrome framework, with a stepped escalation protocol clearly defined for the first time.
How Do the New Treatments Work? — Mechanism of Action
The 2026 guidelines formalise a stepwise pharmacotherapy escalation that uses four classes of lipid-lowering drugs in sequence. Here is how each works:
Pharmacotherapy Escalation — Step by Step
- Step 1 — High-intensity statin (atorvastatin 40–80 mg, rosuvastatin 20–40 mg): Inhibit HMG-CoA reductase, the rate-limiting enzyme in hepatic cholesterol synthesis. Upregulate LDL receptors. Reduce LDL-C by 40–55%.
- Step 2 — Add ezetimibe: Blocks NPC1L1 transporter in the small intestine, reducing cholesterol absorption. Reduces LDL-C by an additional 18–25%.
- Step 3 — Add bempedoic acid (Nexletol): Inhibits ATP-citrate lyase (ACL) upstream of HMG-CoA reductase. Works in the liver, not in muscle — therefore avoids statin-like myopathy. Reduces LDL-C by 21–24%.
- Step 3 (alternative) — PCSK9 monoclonal antibody (evolocumab, alirocumab): Blocks PCSK9, the protein that degrades LDL receptors. More LDL receptors = more LDL removed from blood. Reduces LDL-C by 50–60% on top of statin therapy.
- Step 4 — Inclisiran (Leqvio): siRNA therapy that silences the hepatic PCSK9 gene — prevents the protein being made at all. Only 2 injections/year after loading doses. Reduces LDL-C by 48–52%.
Special Lipid Targets — Beyond LDL
- Triglycerides ≥ 150 mg/dL: Treated with lifestyle first, then fenofibrate or icosapent ethyl (Vascepa) — a purified EPA omega-3 shown in the REDUCE-IT trial to reduce cardiovascular events.
- Lipoprotein(a): Currently no approved Lp(a)-specific drug. PCSK9 inhibitors reduce Lp(a) by 20–30% as a secondary effect. RNA-targeted Lp(a) therapies are in late-stage Phase 3 trials.
- ApoB: Not a drug target directly, but used to guide treatment intensity — particularly in patients with diabetes, obesity, or low LDL where atherogenic burden may be underestimated.
Key Benefits & Clinical Evidence
- LDL targets restored — and lowered: For very-high-risk ASCVD patients, the new target is < 55 mg/dL — a level previously only recommended by European guidelines. Clinical trials show each 38 mg/dL reduction in LDL-C reduces major cardiovascular events by approximately 22%.
- PREVENT replaces PCE: The new AHA PREVENT risk calculator corrects the well-documented 40–50% overestimation of 10-year risk by the old Pooled Cohort Equations. It covers ages 30–79, adds 30-year estimates, and removes race as a variable.
- Earlier intervention: Statins are now considered for patients aged ≤ 30 with familial hypercholesterolaemia, LDL ≥ 160 mg/dL, or a 30-year PREVENT risk ≥ 10% — decades earlier than previous guidelines.
- Universal Lp(a) testing: Every adult should have Lp(a) measured once. Elevated Lp(a) (≥ 50 mg/dL) affects 20–25% of the population and is entirely missed by standard LDL testing.
- Bempedoic acid CLEAR OUTCOMES trial: In patients who cannot tolerate statins, bempedoic acid reduced cardiovascular events — filling a critical gap for the ~10% of patients with statin-attributed muscle symptoms.
- VESALIUS-CV trial (post-guideline): Adding evolocumab (PCSK9 inhibitor) to statin therapy in high-risk patients without prior MI/stroke drove LDL-C to ~45 mg/dL and significantly reduced CHD deaths, MIs, and strokes.

Dosage & Administration — Key Medications
The 2026 guidelines recommend the following evidence-based lipid-lowering agents with these standard dosages:
| Parameter | Details |
|---|---|
| Drug class | Statins (HMG-CoA reductase inhibitors) — first-line for all patients |
| Atorvastatin (high-intensity) | 40–80 mg once daily, with or without food |
| Rosuvastatin (high-intensity) | 20–40 mg once daily, with or without food |
| Ezetimibe (add-on) | 10 mg once daily, with or without food, any time of day |
| Bempedoic acid (Nexletol) | 180 mg once daily, orally — for statin-intolerant patients |
| Evolocumab (Repatha) | 140 mg every 2 weeks OR 420 mg monthly, subcutaneous injection |
| Alirocumab (Praluent) | 75–150 mg every 2 weeks, subcutaneous injection |
| Inclisiran (Leqvio) | 284 mg SC injection: day 1, month 3, then every 6 months |
| Icosapent ethyl (Vascepa) | 2 g twice daily with food — for TG ≥ 150 mg/dL on statin |
| Fenofibrate | 145 mg once daily with a meal — for significant hypertriglyceridaemia |
| Storage — statins/ezetimibe | Room temperature, away from moisture and heat |
| Storage — PCSK9 mAbs | Refrigerate (2–8°C); remove 30 min before injecting |
| Missed dose — statins | Take as soon as remembered, unless next dose is due — do not double up |
Pharmacist Tip: Statin Intolerance
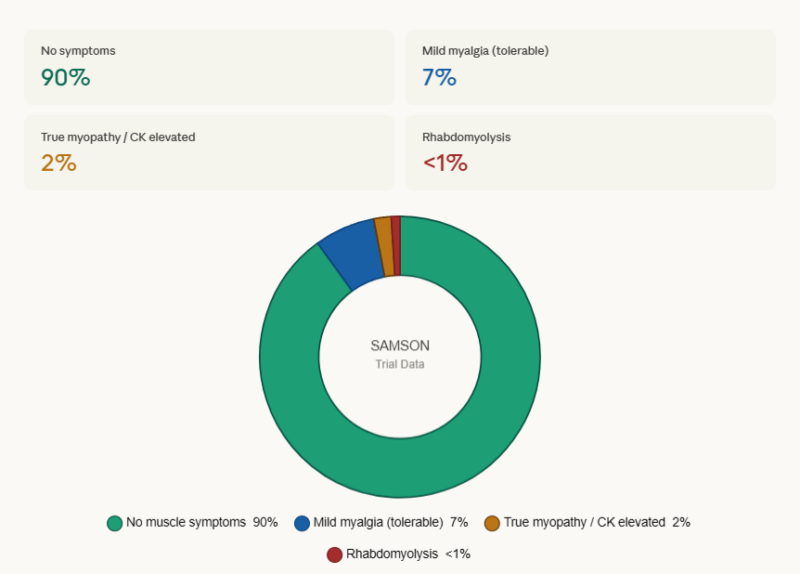
Approximately 10% of patients experience statin-attributed muscle symptoms (SAMS). Key pharmacist counselling points: (1) Confirm true myopathy vs nocebo effect — many patients tolerate statins at lower doses or on alternate days; (2) CK levels > 10× ULN require stopping; (3) Bempedoic acid (Nexletol) is the first evidence-based statin alternative formally recommended in the 2026 guidelines — it does not cause muscle symptoms as it is not taken up by muscle tissue.
Side Effects — What Patients Should Know
Side effect profiles vary by drug class. Below is a summary across the key agents recommended in the 2026 guidelines.
| Common Side Effects (>10%) | Serious Side Effects |
|---|---|
| Statins: muscle aches (myalgia) | Statins: rhabdomyolysis — stop if CK > 10× ULN |
| Ezetimibe: diarrhoea, abdominal pain | Bempedoic acid: tendon rupture (rare, especially with fluoroquinolones) |
| Bempedoic acid: elevated uric acid, gout flare | PCSK9 inhibitors: rarely allergic/anaphylactic reaction |
| PCSK9 inhibitors: injection site reactions | Inclisiran: not for use in pregnancy or severe hepatic impairment |
| Inclisiran: injection site reactions | Statins: contraindicated in pregnancy — stop before conception |
| Fenofibrate: GI upset, elevated creatinine | Fibrates: myopathy risk increases if co-prescribed with statins |
| All agents: liver enzyme monitoring recommended | All classes: interactions with warfarin, cyclosporine — check BNF |
Who Should Be Treated? — Patient Selection
Patients who should start or intensify lipid-lowering therapy
- All adults with established ASCVD (prior MI, stroke, PAD) — target LDL-C < 55 mg/dL
- Adults aged 40–75 with diabetes (type 1 or 2) — statin therapy recommended
- Adults aged 40+ with CKD stage 3 or higher — statin initiation recommended
- Adults aged 40+ with HIV infection — statin therapy recommended
- Adults with familial hypercholesterolaemia (FH) — high-intensity statin, usually from diagnosis
- Primary prevention: 10-year PREVENT risk ≥ 10% — high-intensity statin
- Primary prevention: 10-year risk 5–< 10% (intermediate) — moderate statin after lifestyle trial
- Young adults ≤ 30 with LDL ≥ 160, strong family history, or 30-year risk ≥ 10% — statin considered
- Children aged 9–11: universal cholesterol screening — statin in HeFH or LDL ≥ 160 mg/dL
Contraindications and cautions
- Statins: contraindicated in pregnancy and breastfeeding — stop before conception
- Bempedoic acid: avoid in severe renal impairment (eGFR < 30); monitor for gout in high-risk patients
- PCSK9 inhibitors: no major absolute contraindications, but prior authorisation often required
- Inclisiran: contraindicated in pregnancy; not studied in severe hepatic impairment
- Fibrates: contraindicated in severe renal or hepatic impairment; avoid statin combination in high-risk patients
Important Notice: Always consult a qualified healthcare professional — your doctor, cardiologist, or pharmacist — before starting, stopping, or changing lipid-lowering therapy. The 2026 guidelines require personalised risk discussion. Dosage, monitoring, and drug choice depend on your individual risk tier, comorbidities, and current medications.
Patient Tips & Lifestyle Advice
- Ask your doctor to calculate your 10-year and 30-year ASCVD risk using the new AHA PREVENT calculator — available free at professional.heart.org. This replaces older risk tools and gives a more accurate picture.
- Get your Lp(a) tested at least once. The 2026 guidelines recommend this for every adult — it is a genetically determined risk factor that standard cholesterol panels miss entirely.
- Do not stop statins because of mild muscle aches without first discussing with your pharmacist — the nocebo effect accounts for many perceived symptoms. True statin myopathy is far less common than widely believed.
- Follow a Mediterranean-style or plant-forward diet. These dietary patterns have the strongest evidence for LDL-C and cardiovascular risk reduction. Request a dietitian referral if needed.
- Reduce refined carbohydrates, added sugars, and alcohol — these are the primary dietary drivers of elevated triglycerides, now formally recognised as an independent ASCVD risk factor.
- If prescribed a PCSK9 inhibitor pen (evolocumab or alirocumab), store it in the refrigerator and remove it 30 minutes before injection to reach room temperature — this reduces injection discomfort.
- Children aged 9–11 should have a fasting cholesterol panel at least once. Early detection of familial hypercholesterolaemia is now a guideline priority.
- If you have established heart disease and your LDL is above 55 mg/dL despite statins, ask your cardiologist about adding ezetimibe, bempedoic acid, or a PCSK9 inhibitor — the 2026 escalation pathway is designed for exactly this situation.
Frequently Asked Questions
Q1. What are the new LDL-C targets in the 2026 guidelines?
The 2026 guidelines restore specific LDL-C numerical targets for the first time since 2013. Very-high-risk ASCVD patients (e.g. recent MI, multiple heart attacks) should aim for LDL-C < 55 mg/dL. High-risk ASCVD and high-risk primary prevention patients should aim for < 70 mg/dL. Intermediate-risk and borderline-risk primary prevention patients should aim for < 100 mg/dL. These targets align U.S. recommendations with European guidelines for the first time.
Q2. What is the PREVENT calculator and how is it different from what was used before?
The AHA PREVENT (Predicting Risk of Cardiovascular Disease EVENTs) calculator replaces the old Pooled Cohort Equations (PCE). PREVENT is race-free, covers adults aged 30–79 (vs 40–75 before), provides both 10-year and 30-year risk estimates, includes kidney function (eGFR), and incorporates social deprivation index data. The old PCE was shown to overestimate 10-year risk by 40–50% in many modern populations — leading to overtreatment. PREVENT corrects this.
Q3. What is lipoprotein(a) and why does every adult need to be tested now?
Lipoprotein(a) — or Lp(a) — is a genetically determined atherogenic particle that is causally associated with heart attack and stroke, independently of LDL-C. It affects approximately 1 in 5 people at elevated levels (≥ 50 mg/dL) and is almost entirely unresponsive to statins or dietary changes. The 2026 guidelines recommend that every adult has Lp(a) measured at least once in their lifetime — a landmark universal recommendation that was not in previous guidelines. If elevated, PCSK9 inhibitors (which reduce Lp(a) by 20–30%) or emerging RNA-targeted therapies may be appropriate.
Q4. What is bempedoic acid and why is it now in the treatment pathway?
Bempedoic acid (brand name Nexletol) is an oral cholesterol-lowering drug that works upstream of statins in the cholesterol synthesis pathway. Crucially, it inhibits an enzyme (ACL) that is active in the liver but not in muscle tissue — which means it does not cause the muscle pain (myalgia) associated with statins. The landmark CLEAR OUTCOMES trial, published after the 2018 guidelines, proved that bempedoic acid reduces cardiovascular events in statin-intolerant patients. The 2026 guidelines formally incorporate bempedoic acid into Step 3 of the escalation pathway.
Q5. Are these guidelines relevant to patients already on statins who feel well?
Absolutely. The 2026 guidelines specifically address patients who are on statins but may not be at LDL-C goal. If your LDL-C is above 55 mg/dL (for very-high-risk patients) or above 70 mg/dL (for high-risk patients), the guidelines recommend adding ezetimibe, then bempedoic acid and/or a PCSK9 inhibitor. Many patients and even some clinicians assume that being on a statin means treatment is complete — the 2026 guidelines make clear that reaching the target number matters as much as being on the right drug.
Conclusion
The 2026 ACC/AHA Dyslipidemia Guidelines represent the most ambitious and evidence-based overhaul of cardiovascular lipid management in nearly a decade. For pharmacists and healthcare professionals, the critical messages are clear: start treatment earlier, think beyond LDL to include Lp(a) and ApoB, use the PREVENT calculator for more accurate risk assessment, and escalate therapy along the clearly mapped statin → ezetimibe → bempedoic acid / PCSK9 inhibitor → inclisiran pathway.
For patients, the message is equally important: cardiovascular disease is largely preventable. These new guidelines give clinicians better tools, better targets, and better drugs to help you reach them. Universal Lp(a) testing means millions of people who never knew they were at risk will now be identified and treated. Earlier intervention in young adults and children with familial hypercholesterolaemia means fewer premature heart attacks in the next generation.
Speak with your pharmacist or cardiologist about whether your current lipid management aligns with the 2026 guidelines — and whether your LDL-C, Lp(a), and triglycerides have been assessed comprehensively.
Disclaimer: The information in this blog is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before starting, stopping, or changing any medication. 24x7Pharma does not diagnose, prescribe, or replace professional medical guidance. Guideline summaries are based on the 2026 ACC/AHA/Multisociety Guideline published in JACC and Circulation, March 13, 2026.